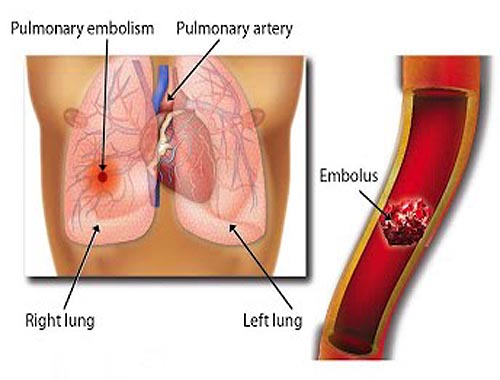
Pulmonary Embolism
Pulmonary embolism is a common and potentially lethal condition. Most patients who succumb to pulmonary embolism do so within the first few hours of the event. Despite diagnostic advances, delays in pulmonary embolism diagnosis are common and represent an important issue. As a cause of sudden death, massive pulmonary embolism is second only to sudden cardiac death. In patients who survive a pulmonary embolism, recurrent embolism and death can be prevented with prompt diagnosis and therapy. Unfortunately, the diagnosis is often missed because patients with pulmonary embolism present with nonspecific signs and symptoms. If left untreated, approximately one third of patients who survive an initial pulmonary embolism die from a subsequent embolic episode. When a pulmonary embolism is identified, it is characterized as acute or chronic. In terms of pathologic diagnosis, an embolus is acute if it is situated centrally within the vascular lumen or if it occludes a vessel (vessel cutoff sign) (see the first image below). Acute pulmonary embolism commonly causes distention of the involved vessel. An embolus is chronic if it is eccentric and contiguous with the vessel wall (see the second image below), it reduces the arterial diameter by more than 50%, evidence of recanalization within the thrombus is present, and an arterial web is present.