Diabetes Insipidus
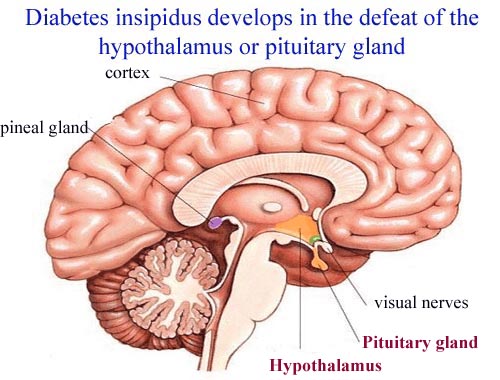
The disorder characterized by intense thirst and the excretion of large amounts of urine (polyuria). In most cases, it's the result of your body not properly producing, storing or releasing a key hormone, but diabetes insipidus (DI) can also occur when your kidneys are unable to respond properly to that hormone. Rarely, diabetes insipidus can occur during pregnancy (gestational diabetes insipidus). Diabetes insipidus (DI) may be central or nephrogenic. Central DI is characterized by decreased secretion of antidiuretic hormone (ADH)-also known as arginine vasopressin (AVP)-which gives rise to polyuria and polydipsia by diminishing the patient's ability to concentrate urine. Diminished or absent ADH can be the result of a defect in 1 or more sites involving the hypothalamic osmoreceptors, the supraoptic or paraventricular nuclei, or the supraopticohypophyseal tract. In contrast, lesions of the posterior pituitary rarely cause permanent diabetes insipidus, because ADH is produced in the hypothalamus and still can be secreted into the circulation. Nephrogenic DI is characterized by a decrease in the ability to concentrate urine due to a resistance to ADH action in the kidney. Nephrogenic DI can be observed in chronic renal insufficiency, lithium toxicity, hypercalcemia, hypokalemia, and tubulointerstitial disease; rarely, diabetes insipidus may be hereditary. Pharmacologic treatment of DI generally involves the use of desmopressin (1-deamino-8-D-arginine vasopressin [DDAVP]), nonhormonal drugs, or both. Patients must be instructed in simple principles of water balance to avoid dehydration and water intoxication (if not carefully monitoring water intake).